


Radiofrequencies and health : where are we ?
PDF
Mobile telephony and new wireless communication technologies have developed exponentially since the 1990s. At the same time, fears have arisen about the possible harmful effects of electromagnetic waves such as radio frequencies on health. We hear everything and its opposite on this subject. For health agencies, the use of these waves is the subject of attention, but does not seem to pose a problem insofar as their use is regulated. They rely on collective expert reports that analyze in detail the available scientific literature to assess the risk. The regulations are based on scientific evidence. However, a number of press articles, radio and television broadcasts, videos and websites regularly report on the dangers. Radio frequencies are said to be carcinogenic, dangerous for children, for fertility, for immunity, etc. The 5G would be a new threat. Testimonies of so-called “electrosensitive” or “electrohypersensitive” (EHS) people are relayed. What exactly is the situation? What are the risks? How are they assessed and regulated? This article offers an overview of the subject based on the case of mobile telephony.
1. The waves that surround us: what are they?
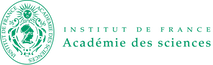
We live within magnetic and electromagnetic fields of multiple origins, natural and artificial. Light, ultraviolet (UV) and infrared (IR) radiation emitted by the sun, and the earth’s magnetic field are determining factors for life on earth. Light, infrared and UV can also be produced artificially. For example, all warm bodies emit IR radiation, whether they are living beings, a radiator in a room, a stone heated by the sun… The sources of radiation have diversified with the establishment of the electrical distribution network. New low-frequency electric and magnetic fields (50 Hz, 60 Hz and their harmonics) then appeared in the environment, followed by radio frequencies, only a very small proportion of which are of natural origin and come from the cosmos [1]. For more than a hundred years, it has been known that all these radiations are associated with a wide range of physical phenomena and effects that differ according to the characteristics of the radiation considered. They are used for a wide range of applications, not only in everyday life, but also for medical, industrial and military purposes (Figure 1).
Interactions with living organisms differ according to the frequency. Up to 100 kHz, fields and currents can stimulate excitable tissues (nervous systems and muscles). Above 10 MHz, absorption by the tissues becomes predominant and heating the essential mechanism. At the so-called intermediate frequencies, between 100 kHz and 10 MHz, there is a mixture of both (Figure 2).

1.1. What happens when radio waves reach the body?
Waves are both reflected by the body (about 50% reflection around GHz) and absorbed within biological tissue. The depth of penetration and the effects of electromagnetic waves differ according to the frequency. This absorption depends on many parameters: temperature, physico-chemical characteristics of the material (permittivity, conductivity, density), exposure level (incident power), type of signal, etc.
In the radio frequency range
The higher the frequency, the less the waves penetrate the body, their absorption is limited to the skin from about 6 GHz. The quantities that account for exposure at body level are therefore not the same. Below 6 GHz, the penetration depth can reach several centimetres. The specific absorption rate (SAR) is the quantity that represents the amount of energy absorbed per unit of mass (in watts per kilogram, W/kg). Since the penetration of waves varies with frequency, the amount of energy absorbed, and therefore the resulting SAR, also varies with frequency for the same incident power. The SAR value is obtained by biological dosimetry using physical measurements and numerical simulation methods. The maximum absorption is around 80 MHz for the human body. Above 6 GHz, the absorption of the waves is increasingly superficial at the skin level. The exposure indicator is the absorbed power density (Sab) in watts per square meter (W/m2) for localized exposures. However, sufficiently intense surface exposures over the whole body could eventually lead to deeper heating. SAR therefore also remains an indicator for the whole body (a consideration introduced in the latest ICNIRP recommendations in 2020, see focus Radiofrequencies, risk and regulation).
1.2 Thermal effects of radio frequencies and critical thresholds
It has been known for a long time that the interaction of RF with matter leads to heating, mainly due to the agitation of water molecules. The higher the water content, the greater the temperature increase. This is known as a threshold effect because this phenomenon occurs after a certain amount of energy has been absorbed, i.e. after a certain level of exposure. This effect is used in many applications: microwave ovens, surgery, industrial thermobonding for example (tarpaulins, blinds…). Mammals have a temperature regulation system that can cope with variations of a few degrees Celsius. Heat is eliminated largely through the vascularization of tissues by normal physiological processes of thermoregulation. A potentially harmful thermal effect occurs when this adaptive capacity is exceeded, starting at critical thresholds. The first effects observed are behavioural disorders in fully exposed primates, and for localised exposures, burns and cataracts, as the eye has very little vascularisation. The critical SAR values derived from scientific data (animal experiments) are:
– 4 W/kg for “whole body” exposure
– 100 W/kg for localized exposure (on average on 10 g of tissue)
For wireless communications, the exposure levels are low enough not to induce heating due to the waves (see focus Some preconceived ideas). There are regulations that set exposure limits that must not be exceeded to protect the population (Read focus Radiofrequencies Risk and Regulation). To study the effects of radio waves in the laboratory, the nuance “near field” / “far field” is important to define the conditions and the exposure system to be used according to the objective of the study (whole body or localized exposure).
2. From research to risk assessment – state of knowledge
2.1. Why conduct research if the effects are known?
Since the 1980s, research has focused on the possible non-thermal effects of radio frequencies. These are effects that are not caused by a change in temperature and occur at low levels of exposure, below critical thresholds. Fears about possible harmful effects of mobile phones were expressed as early as 1993 with a well-publicised trial in the USA. A manufacturer was accused of being responsible for the death of a woman suffering from a brain tumour [2]. On the other hand, for more than 20 years, the installation of telephone antennas has led to debates in which risks for the health of local residents are often put forward [3].
Mobile phones are the main source of exposure to radiofrequencies for the population, due to their positioning close to the head or body during communications, and their widespread use. The SARs generated are well below the critical thresholds, but mobile phones have introduced a new exposure situation (see focus Radiofrequencies risks and regulations). Instantaneous exposure to the phone is tens of thousands of times higher than that generated by antennas, in terms of SAR.
Given the popularity of this technology, the hypothesis of a health risk, even if small, has been taken seriously. For these reasons, most of the studies concern exposure to mobile telephony in the frequency bands concerned. This work allows for a regular assessment of the risk and the relevance of regulatory thresholds. As technologies are constantly evolving, the resulting conditions of exposure of individuals are also evolving. This may give rise to new questions, rumours or opposition, as is currently the case with the arrival of 5G.
2.2. Why are the methods used in research so controversial?

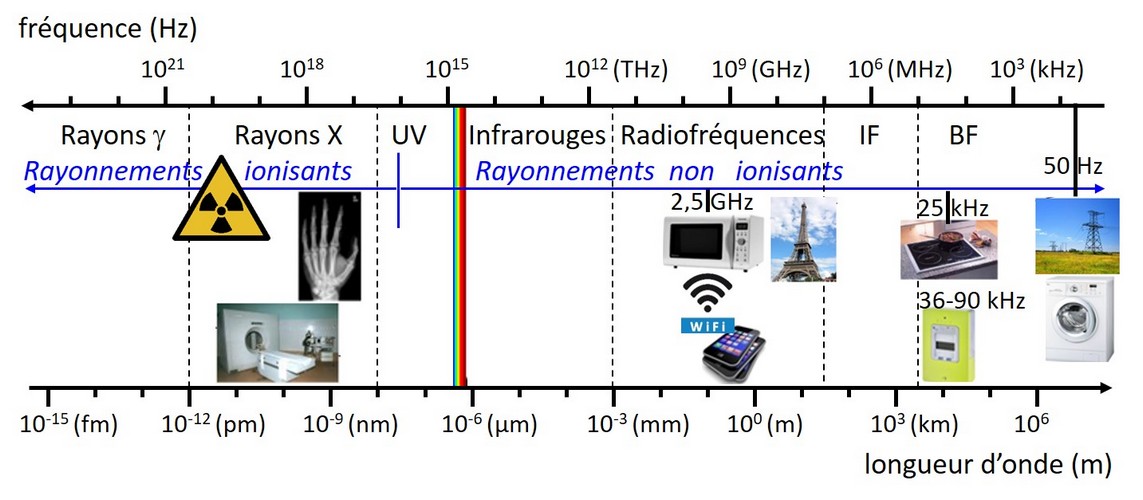
Numerous studies have been conducted on cultured cells, animal models and humans. The aim is to examine whether biological and physiological effects or diseases can be induced, modified or aggravated by radio waves. Experiments have also been carried out on animals exposed to radio frequency radiation on a one-off basis or throughout their lives, including from the gestation period. Table 1 summarizes the number of studies on the biological and health effects of radio frequencies used in wireless communications, including studies in the humanities and social sciences.
- In the laboratory
As with other toxicological studies, the experiments are designed to compare what happens in the presence (or absence) of the risk factor of interest, in this case RF.
It is essential to know the SAR value in the frequency bands concerned, or the incident power absorbed at the surface at higher frequencies. Controlling the exposure characteristics, including SAR, is the main difficulty in these studies. This is more complicated than in “classical” toxicology, where researchers test different doses of a substance (quantified in grams administered per kilogram, for example). Waves cannot be weighed… The exposure system must be adapted and sized [4]. For example, placing a telephone on a rat, on a box containing sperm or on eggs, placing animals in front of a microwave oven with a broken door or a television, as has already been done, are among the most crude errors. The presence of the waves should be the only parameter that differs between samples, animals, or exposed volunteers and controls. Unexposed controls (called “shams“) should therefore be placed under identical conditions but with the transmitter turned off. The specific biases in this field of research are difficult to spot when reading a scientific article because it requires expertise in physics, biology and bioelectromagnetism.
- In the population
Epidemiological studies aim to find a link between disease and exposure. There are two types of epidemiological studies. Case-control studies, in which people suffering from a disease whose cause is being investigated are included. Exposure assessment is generally based on the participants’ memories. Recall bias can distort the results, particularly in remote situations or when the respondents are relatives of sick or dead people. Conversely, cohort studies aim to compare the evolution of pathologies or the health of individuals over time, in more or less exposed populations. Here again, the evaluation of the actual exposure of subjects to radiofrequency waves is delicate because it also depends on the chosen indicator (duration of communication, positioning of the telephone, telephone subscriptions, etc.). Environmental parameters related to lifestyles or specific to individuals may play a role in health status (confounding factors) and must also be taken into account [5].
Interpreting the results of population-based studies is complicated. In general, these studies do not identify small-scale effects in certain subgroups. For wave effects, collaboration with physicists specialised in biological dosimetry can be useful to best assess exposure levels and the larger the sample size, the more conclusive the study result will be.
- Has there been much research in this area?
2.3. How is risk assessed?
Risk is assessed based on all the scientific data published worldwide. For this purpose, health agencies or reference institutions bring together groups of specialists from various backgrounds (biologists, physicians, epidemiologists, physicists, etc.). They take stock of the state of knowledge and produce collective expert reports. The data analysis method follows a rigorous process that is specified in the reports. In the media, effects observed in one study and then not confirmed later are regularly reported without nuance or contextualization in relation to the data as a whole. Rebuttals, when they do occur, are very rarely reported [6]. Moreover, it is always possible to publish an article in a scientific journal, particularly in generalist journals or those not specialised in bio-electromagnetism, even if its content is dubious [7]. It is therefore preferable to refer to collective expert reports and the conclusions of agencies.
We will come back to a few important subjects with a high media impact: the IARC classification and children’s exposure. Read also the focus associated with this article on 5G, on the study of the National Toxicology Program (USA) and on electromagnetic hypersensitivity.
3. Cancer, epidemiology and IARC classification
3.1. Why study the potential effect of RF on cancer?
Identifying the causes of cancer is an important issue in public health [8]. Among the many factors influencing the development of cancer pathology (from initiation to clinical evidence, sometimes years later), mechanisms leading to DNA damage play an important role. The energy carried by radio frequencies is not sufficient to directly cause breaks in DNA molecules. No mechanism that could explain such a biological effect is currently described. Nevertheless, the question of a possible effect of RF on the integrity of genetic material and on carcinogenesis has been, and still is, extensively studied. On the other hand, epidemiologists have been looking for an association between cancers and RF, in particular between mobile phone use and brain tumours.
3.2. IARC classification of radio frequencies
Collective reviews conducted by the International Agency for Research on Cancer (IARC, the cancer agency of the WHO) are concerned only with studies that may indicate that an agent is carcinogenic. This can be chemical or natural substances, food, physical agents (waves…) or an occupational situation (e.g. firefighter) to which humans are likely to be exposed. IARC explicitly distinguishes between risk and hazard. The classification takes into account the level of evidence of the existence of a danger, i.e. the carcinogenic character for humans, without quantifying the risk which depends on the conditions of exposure. Thus, asbestos, alcohol, cold cuts and wood dusts, for example, can be placed in the same category. The classification scale used by the IARC [9] is summarised in Table 2.

In 2011, IARC classified radio frequencies as “possibly carcinogenic“, or “possibly carcinogenic“, to humans (2B) in relation to mobile phone use [10]. This is mainly due to the results of the INTERPHONE study[11]. This is the largest case-control study conducted to date on the subject (data from 13 countries), including 2708 gliomas, 2409 meningiomas. The patients were divided into 10 groups according to the cumulative duration of their conversations. An increased risk of glioma brain tumour was found for the group with the longest conversation times over a ten-year period (>1640 h; OR 1.40 (95% CI 1.03-1.89). The authors found some of the reported times (up to 12 hours per day) implausible. Furthermore, there was no increasing association with exposure times. The authors concluded that: “Overall, no increased risk of glioma or meningioma was observed with mobile phone use. There were suggestions of an increased risk of glioma at the highest exposure levels, but bias and error prevent causal interpretation. The possible effects of long-term intensive use of mobile phones need further study“.
The results were similar for acoustic neuroma but based on few cases. A publication by Hardell et al [12] was also important for classification, although it was limited in scope and had limitations [13]. Note that a case-control study (“Cerenat”) [14], covering 4 regions in France, caused a media wave in 2014 [15]. It is sometimes presented as the confirmation of the INTERPHONE study. Indeed, no association between mobile phone use and the occurrence of brain tumours was observed, except for gliomas in the heaviest users. The “heavy users” group corresponds to the 10% of people who reported the longest cumulative communication times in each study. Their comparison is delicate since it concerns a cumulative duration of more than 896 h (24 cases) in Cerenat and almost double in INTERPHONE and 4 times as many cases (> 1640 h, 100 cases) where no increase in risk is observed for durations less than 1640 h. It should also be kept in mind that the power of this study (253 glioma cases included) is low compared to INTERPHONE (2708 glioma cases) and that it has a number of biases [16]. On the other hand, cohort studies have not provided evidence in favour of a carcinogenic effect of mobile phones, including one conducted in Denmark [17] which followed 358,403 people for 18 years. Exposure was assessed on the basis of the participants’ telephone subscriptions, without specifying the duration of conversations. Another important cohort study is the Million women study [18], which was published after the IARC classification. Conducted in Great Britain on about 800,000 women followed for 7 years, it did not show any association between mobile phone use and an increased incidence of gliomas, meningiomas and 18 other types of cancers.
Ultimately, the IARC classification is often understood as evidence of the carcinogenicity of radio frequencies. However, RF has not been found to be a probable or proven human carcinogen by IARC, which is consistent with the conclusions of the collective reviews and the WHO position [19].
3.3. Has the number of cancers increased with mobile phone use?
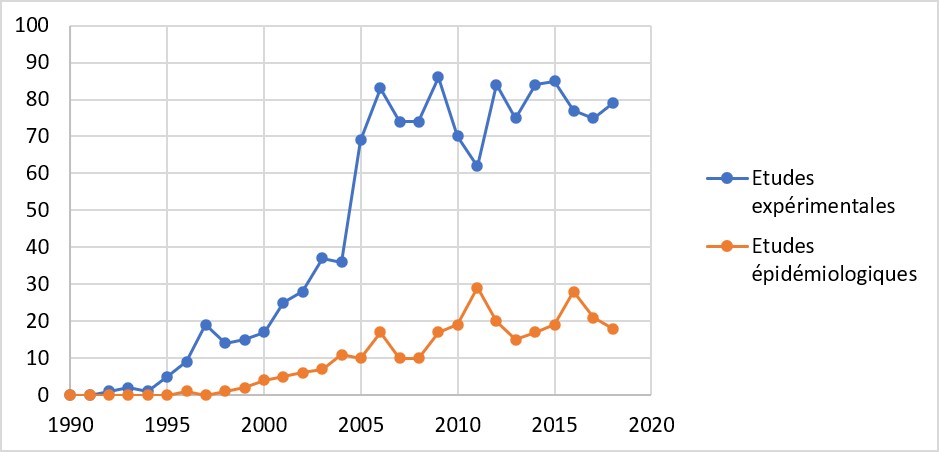
Since 2004, and especially after the IARC classification, researchers have been looking for a link between the evolution of the incidence of brain tumours (number of new cases per year per 100,000 inhabitants) over time, in particular gliomas, and mobile phone use in the population. More than ten studies have been conducted using data from national cancer registries in 13 countries (USA, Great Britain, China, Nordic countries, Denmark, New Zealand, Taiwan, Australia, Japan, Italy, Israel, Sweden, Finland), resulting in more than 25 scientific publications [20]. Depending on the study, variations in incidence have been observed over time or not. They generally appear to be related to changes in the frequency of screening and/or improvements in the methods of screening and analysis of tumours [21]. In any case, these variations do not correspond to those expected if the associations (relative risks) reported in the studies at the origin of the IARC classification were real, as illustrated by the graphs taken from one of these studies (Figure 4) [22].
4. Children’s exposure

It should be noted in passing that the Academies of Science, Medicine and Technology have examined the use of screens by children and adolescents, calling for reasoned vigilance regarding digital technologies [25].
5. Assessment of the state of knowledge
5.1. What do we know about risk?
In 2012, following the analysis of 33 reports published between 2009-2011 [26], Luc Verscheave, a toxicologist then member of the Belgian Scientific Institute of Public Health, wrote “All reports, with the exception of the BioInitiative report, conclude that there is no clear evidence of adverse health effects from exposure to radio frequencies from applications used for wireless communication. They remain generally cautious about long-term biological effects, not because of strong indications that such effects might occur, but only because of the lack of data available so far to draw a meaningful conclusion.” [27]
Note that in 2013, as in 2009, the French Agency for Health Safety, Food, Environment and Work (Anses) invited to consider the “Bioinitiative” report [28] with caution because “it conceals conflicts of interest in several sections, does not correspond to a collective expertise, is of uneven quality according to the sections, and is written in an activist register.” [29], which is in line with other analyses [30]. Since 2012, new expert reports have been produced in France (2013), the Netherlands (2016) [31] in Sweden (2018) [32] at the European level (2015) [33] Australia (2017) [34] in the USA (2020, focused on cancer) [35] for example, without bringing any substantial change to the state of knowledge. It appears that the studies with the highest risk of bias more often report effects, and it is then difficult to identify the origin of these effects. Conversely, those with good exposure characterization rarely suggest a significant effect at non-thermal exposure levels. There are always a few studies considered of good quality that show biological or physiological effects, sometimes even beneficial effects. These disparate results are considered limited evidence until the effects are demonstrated by a consistent and reproducible set of results. To date, the conclusions of scientific expert reports from around the world are consistent. They do not indicate a proven health risk from radio frequencies, nor do they indicate a biological mechanism that may underlie a risk for exposures within regulatory limits.
5.2. Is there any ongoing research?
The period of intense research on the subject is now over. Research is continuing more or less actively depending on the country. In France, the ANSES funds research projects every year. Two major epidemiological studies are underway for long-term exposure, over 15 years.
- COSMOS study: involves about 300,000 people followed in 6 European countries, for 20-30 years, to study a possible association between health problems and the use of mobile phones or other wireless technologies.
- MOBI-KIDS study (14 countries): the aim is to assess the potential link between brain tumours in children and young adults (10-24 years) and environmental risk factors, including the use of mobile communications.
A special effort is being made to characterize exposure, which has often been a weak point in this type of study. The arrival of 5G should give rise to a new wave of research, especially in the millimetre frequency bands around 26 GHz where there are few studies compared to the frequencies close to those already used for mobile telephony and WiFi. It therefore seems likely that few new studies will be conducted around 3.5 GHz.
6. Bringing elements of response

The issue of radio frequency risk and wireless communications has multiple dimensions, from scientific and technical to societal and political. The development of these technologies in everyday life has had, and will continue to have, major repercussions on habits and lifestyles. This explains the multiple facets of the controversies surrounding the new wireless communication technologies, where questions related to health aspects and the use of the technologies are intertwined with environmental and economic issues. A lot of erroneous information, “infoxes”, and even rumours circulate on the supposed dangers of waves, to defend causes, sell services or so-called “anti-wave” protection, become famous, oppose new technologies, satisfy an electorate, fight a battle… However, the media are fond of sensational news. They often contribute to the confusion by presenting all types of information on these subjects on the same level, whether they are scientifically validated or opinion based (Figure 6). In this context, scientific risk assessments are not intended to resolve controversies or dictate what should be done. On the other hand, science provides answers that enable decision-makers to take appropriate public health measures, among other things, and citizens to form an opinion. And, as with other health-environment issues, the most difficult thing is to sort through the information.
7. Messages to remember
Concerning the health aspects, we will retain that:
- In the radio frequency range, the results of the scientific work conducted to date have not demonstrated the existence of a harmful effect, nor a plausible biological mechanism that could underlie a risk below the regulatory limit values.
- The only known effect of radio frequencies is the thermal effect at high levels of exposure, which is not achieved with wireless technologies.
- With regard to the effects of electromagnetic fields, the WHO considers that “the scientific knowledge acquired in this field is now more complete than that which we have on most chemicals” [36].
- In science, it is all a question of probability and level of proof. It is impossible to scientifically demonstrate an absence of effect, so an absence of risk will never be demonstrated, whatever the risk factor.
The media and social networks readily relay alarming testimonies and messages on the effects of waves based on an isolated study or hasty interpretations, or even on pure and simple allegations.
- Considering the subject in its entirety, beyond the health issue, makes it possible to grasp the issues involved and to better decipher the information.
- It is useful to cross-reference sources of information and to sharpen one’s critical mind in order to remain free in one’s opinion.
I would like to thank Catherine Yardin and Isabelle Lagroye for their careful review and comments on the biological and health aspects, and Allal Ouberehil on the technical aspects of wireless communications.
Notes and references
Cover image. [Source: Leon Brooks, Public domain, via Wikimedia Commons – Tim Parkinson, CC BY 2.0 <https://creativecommons.org/licenses/by/2.0>, via Wikimedia Commons]
[1] EMF-portal, Natural radio frequency fields.
[2] Lawsuit claims cellular phones cause cancer, UPI archives, 3 January 1993.
[3] Borraz O., Devigne M., Salomon D., Controverses et mobilisations autour des antennes de téléphonie mobile, 2004, Rapport du centre de sociologie des organisations, 160 p.
[4] Kuster and Schönborn. 2000, Recommended minimal requirements and development guidelines for exposure setups of bio-experiments addressing the health risk concern of wireless communicationsBioelectromagnetics, 21:508-514.
[5] Souques M., Notions de base sur l’épidémiologie, 2009, SPS n° 286, July 2009. On afis.org
[6] See the dossier “Science and the media” in Science et Pseudosciences n°323 of the Association pour l’Information scientifique. On afis.org
https://www.afis.org/-323
[7] See the articles of H. Maisonneuve on afis.org/Herve-Maisonneuve
[8] Hill C., 2019, What do we know about the causes of cancer?
[9] https://monographs.iarc.fr/agents-classified-by-the-iarc/
[10] IARC Press Release, 31 May 2011
Full report published in 2013: IARC, 2013, Non-ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 102.
and IARC, 2013, Non-ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 102.
[11] THE INTERPHONE Study GROUP et al. (2010) Brain tumour risk in relation to mobile telephone use: results of the Interphone international case-control study. International J. Epidemiology 39(3):675-694.
[12] Hardell L, Carlberg M, Hansson Mild K. Pooled analysis of case-control studies on malignant brain tumours and the use of mobile and cordless phones including living and deceased subjects. Int J Oncol 2011; 38: 1465-74.
[13] Ahlbom et al, Epidemiologic Evidence on Mobile Phones and Tumor Risk: A Review (Epidemiology 2009; 20: 639-652)
[14] Coureau & al, 2014, Mobile phone use and brain tumours in the CERENAT case-control study. Occup Environ Med, 71(7):514-22.
[15] Mobile phone and tumor, what is the link? – Deciphering a recently published epidemiological study on the effects of telephone radio frequencies on the brain, and a look back at the over-mediation that has agitated the web with Dr Gaëlle Coureau. 22 May 2014, University of Bordeaux. On https://www.u-bordeaux.fr/
[16] Mobile phones and brain cancers: double zero score for Bordeaux study, 23 May 2014. Journalism and public health – The blog of Jean-Yves Nau, journalist and medical doctor. On jeanyvesnau.com
[17] Frei P et al Use of mobile phones and risk of brain tumours: update of Danish cohort study. BMJ 2011; 343: d6387. doi: 10.1136/bmj.d6387
[18] Benson VS et al Mobile phone use and risk of brain neoplasms and other cancers: prospective study. Int J Epidemiol 2013; 42: 792-802.
[19]Electromagnetic fields and public health: mobile phones, 8 October 2014
[20] These studies are listed in the EMF-Portal database, under Mobile communication, population studies, brain cancer. https://www.emf-portal.org/en/article/overview/mobile-communications-epidem/brain-cancer#level-2
[21] As an example, see reading note on the Australian publication released in late 2018:
https://www.afis.org/Telephone-mobile-et-tumeurs-cerebrales-quoi-de-neuf
[22] Chapman S. & al., 2016, Has the incidence of brain cancer risen in Australia since the introduction of mobile phones 29 years ago? Cancer Epidemiology, 42:199-205
[23] HCB, 2011, Influence of radiofrequency telecommunication signals on children’s brains.
[24] ANSES, report “Exposure to radio frequencies and children’s health”, June 2016. https://www.anses.fr/fr/search/site/rapport%20radiofr%C3%A9quences?searchphrase=1&mm=100&iso1=fr&iso2=en
[25] Academy of Sciences, New call “The child, the adolescent, the family and the screens”, Press release of 9 April 2019.
https://www.academie-sciences.fr/fr/Communiques-de-presse/enfant-adolescent-famille-ecran.html
[26] Verschaeve L., Evaluations of International Expert Group Reports on the Biological Effects of Radiofrequency Fields, Wireless Communications and Networks, 2012, Recent Advances, Dr. Ali Eksim (Ed.), ISBN:978-953-51-0189-5, InTech. (translation and citation, A. Perrin).
[27] https://cdn.intechopen.com/pdfs/31625/InTech-Evaluations_of_international_expert_group_reports_on_the_biological_effects_of_radiofrequency_fields.pdf
[28] https://bioinitiative.org/
[29] Anses, update of the ” Radiofrequencies and health ” expertise, October 2013, http://www.anses.fr/sites/default/files/documents/AP2011sa0150Ra.pdf
[30] https://fr.wikipedia.org/wiki/Bioinitiative
[31] Health council of Netherlands, 2016, Mobile phones and cancer, Part 3. Update and overall conclusions from epidemiological and animal studies
[32] Scientific Council of Swedish Radiation Safety Authority (SSM), 2018,
[33] SCENIHR, “Potential health effects of exposure to electromagnetic fields (EMF)”, March 2015. Summary sheet: http://ec.europa.eu/health/scientific_committees/docs/citizens_emf_fr.pdf
[34] Australian Radiation Protection Agency (ARPANSA), 2017,
Technical Report “Radiofrequency Electromagnetic Energy and Health: Research Needs, TR178
[35] Food and drug Administration (USA), 2020, Review of Published Literature between 2008 and 2018 of Relevance to Radiofrequency Radiation and Cancer. https://www.fda.gov/media/135043/download
[36] WHO, Electromagnetic fields – Summary of health effects https://www.who.int/peh-emf/about/WhatisEMF/fr/index1.html
The Encyclopedia of the Environment by the Association des Encyclopédies de l'Environnement et de l'Énergie (www.a3e.fr), contractually linked to the University of Grenoble Alpes and Grenoble INP, and sponsored by the French Academy of Sciences.
To cite this article: PERRIN Anne (January 5, 2025), Radiofrequencies and health : where are we ?, Encyclopedia of the Environment, Accessed April 8, 2025 [online ISSN 2555-0950] url : https://www.encyclopedie-environnement.org/en/health/radiofrequencies-health/.
The articles in the Encyclopedia of the Environment are made available under the terms of the Creative Commons BY-NC-SA license, which authorizes reproduction subject to: citing the source, not making commercial use of them, sharing identical initial conditions, reproducing at each reuse or distribution the mention of this Creative Commons BY-NC-SA license.


